Please cite this article as: E C, P C, R R, I L, R Z, G D, O A, V L, G MC, F F, FJ Cdl, JA GH, A AS. Geriatric assessment for predicting outcomes among patients with aortic stenosis undergoing transcatheter aortic valve implantation. J Geriatr Cardiol 2025; 22(5): 516−524. DOI: 10.26599/1671-5411.2025.05.005.
Citation:
Please cite this article as: E C, P C, R R, I L, R Z, G D, O A, V L, G MC, F F, FJ Cdl, JA GH, A AS. Geriatric assessment for predicting outcomes among patients with aortic stenosis undergoing transcatheter aortic valve implantation. J Geriatr Cardiol 2025; 22(5): 516−524. DOI: 10.26599/1671-5411.2025.05.005.
Please cite this article as: E C, P C, R R, I L, R Z, G D, O A, V L, G MC, F F, FJ Cdl, JA GH, A AS. Geriatric assessment for predicting outcomes among patients with aortic stenosis undergoing transcatheter aortic valve implantation. J Geriatr Cardiol 2025; 22(5): 516−524. DOI: 10.26599/1671-5411.2025.05.005.
Citation:
Please cite this article as: E C, P C, R R, I L, R Z, G D, O A, V L, G MC, F F, FJ Cdl, JA GH, A AS. Geriatric assessment for predicting outcomes among patients with aortic stenosis undergoing transcatheter aortic valve implantation. J Geriatr Cardiol 2025; 22(5): 516−524. DOI: 10.26599/1671-5411.2025.05.005.
There is scarce data about comparisons between geriatric assessment tools in patients with aortic stenosis (AS). We aimed to describe the geriatric profile of patients with AS undergoing transcatheter aortic valve implantation (TAVI) and to analyze the ability of different tools for predicting clinical outcomes in this context.
Methods
This was a single center retrospective registry including patients with AS undergoing TAVI and surviving to hospital discharge. The primary endpoint was all-cause mortality or need for urgent readmission one year after TAVI.
Results
A total of 377 patients were included (mean age of 80.4 years). Most patients were independent or mildly dependent, with an optimal cognitive status. The proportion of frailty ranged from 17.6% to 49.8%. A total of 20 patients (5.3%) died and 110/377 patients (29.2%) died or were readmitted during follow up. Overall, most components of the geriatric assessment showed an association with clinical outcomes. Disability for instrumental activities showed a significant association with mortality and a strong association with the rate of mortality or readmission. The association between frailty and clinical outcomes was higher for short physical performance battery (SPPB), essential frailty toolset (EFT) and the frailty index based on comprehensive geriatric assessment (IF-VIG) and lower for Fried criteria and FRAIL scale.
Conclusions
AS patients from this series presented a good physical performance, optimal cognitive status and a reasonably low prevalence of frailty. The best predictive ability was observed for disability for instrumental activities and frailty as measured by the EFT, SPPB and the IF-VIG.
In recent years, the transcatheter aortic valve implantation (TAVI) procedure has increased exponentially among patients with aortic stenosis (AS). Although the indications have expanded to younger ages and lower-risk patients, to date candidates for TAVI are still usually elderly patients with a significant burden of comorbidities. The benefit of TAVI in these complex patients might be lower -or even disappear- as compared to robust patients without comorbidities.[1] In this sense, optimizing selection of patients in order to avoid futility is still a real clinical challenge.
During the first years of TAVI development risk was mostly calculated by using surgical scores. However, among older patients with AS a multidimensional assessment of the patient is especially important, taking into account their biological age by a comprehensive geriatric assessment. This strategy is to date strongly recommended by the different scientific societies.[2,3] Frailty and the rest of the components of the geriatric evaluation are associated with poorer outcomes in older patients with cardiovascular diseases. Specifically, frailty is one of the strongest predictors of cardiovascular events and mortality in this complex setting.[4-6]
However, implementing a comprehensive geriatric assessment (CGA) in routine clinical practice is difficult for different reasons. There are many types of scales, and there is a significant heterogeneity regarding the tools used in different countries and centers.[7] The most complex tools have usually a better performance for predicting outcomes, but its assessment is time consuming and requires trained professionals, specific spaces and other healthcare resources. With the exponential increase in the number of TAVI procedures worldwide, workload of nurses and allied professionals should be adapted to this increasing demand.[2,5] On the other hand, the predictive ability of these scales is highly variable in different clinical settings. There is scarce data about direct comparisons of the performance of these different scales for predicting clinical outcomes among older patients with AS. Therefore, the main aim of this study was to describe the geriatric profile of a series of older patients with AS undergoing TAVI and to analyze the predictive value of different geriatric assessment tools for predicting one year clinical outcomes in this context.
METHODS
This is a retrospective registry carried out at a public tertiary care Hospital in Spain. We included patients with AS who were visited by the TAVI nurse for a CGA prior of the TAVI procedure, undergoing TAVI and surviving to hospital discharge between January 2020 and October 2023.
Data Collection
Data were retrospectively collected by local investigators using standardized case report forms. Demographics, baseline clinical features, electrocardiographic data and echocardiographic, laboratory and angiographic parameters were collected. In-hospital clinical outcomes were also collected, such as the need of invasive procedures and in-hospital complications.
Comprehensive geriatric assessment
A baseline geriatric evaluation was carried out before the TAVI procedure through an interview with the patient and/or family or caregivers.
● The functional capacity for basic activities of daily living was assessed by the Barthel index[8]. It is an ordinal scale with a total score from 0 to 100, whose intermediate ranges help to evaluate the different degrees of dependence: total (0-20), severe (21–40), moderate (41–60), light (61–90), and independent (> 90).
● Instrumental activities were evaluated by the Lawton-Brody Instrumental Activities Index[9] whose values range from 0 (low function) to 8 (high function) and analyses 8 instrumental daily living activities.
● Cognitive status was evaluated with the Pfeiffer Test[10] was used to assess cognitive impairment. The classification is: Intact Cognitive Functioning (0–2 errors), Mild cognitive impairment (3–4 errors), Moderate cognitive impairment (5–7 errors) and Severe cognitive impairment (8–10 errors).
● Frailty was evaluated by using 5 different tools:
This test includes: (a) balance in three positions (feet together, semi-tandem and tandem), (b) walking speed (4 m) and (c) getting up and sitting down in a chair five times. The SPPB total score is the sum of the three scores, ranging from 0 to 12. A score less than 10 indicates a higher risk of disability and falls.
o FRAIL scale[12] (which includes the evaluation of fatigue, resistance, ambulation, comorbidities and weight loss). Frailty was defined as a clinical syndrome in which three or more of the following criteria were present: unintentional weight loss (5 kg in past year), self-reported exhaustion, weakness (grip strength), slow walking speed, and low physical activity. Frail scale scores range from 0–5 (i.e., 1 point for each component; 0 = best to 5 = worst) and represent frail (3–5), pre-frail (1–2), and robust (0) health status. Frailty was defined by a Frail score ≥ 3 points.
(2) Essential Frailty Toolset (EFT) scale[5] , which includes a) the test of getting up from the chair 5 times, b) the Mini Mental State Examination, c) hemoglobin valuesand d) albumin.
(3) FRIED scale[13] : The Fried scale consists of 5 items, with 3 of 5 required to diagnose frailty: 5-m gait speed, grip strength, weight loss, exhaustion, and inactivity
(4) IF-VIG[14]: It combines in its scale multidimensional Frailty Indexes (IF) with the Comprehensive Geriatric Assessment (CGA). Based on 22 simple and dichotomous questions, to assess 25 deficits.
Clinical outcomes
The primary endpoint for the purpose of this study was all cause mortality or need for urgent readmission after one year of follow up. The assignment of the cause of death was based on clinical judgment of the physician taking care of the patient at the time of death. In cases of coexistence of two or more possible causes, the assignment was performed taking into account the clinical relevance of each of those conditions and their contribution at the time of death. Death was deemed cardiac when it was be due to myocardial infarction, heart failure or sudden death. The number of readmissions and emergency department (ED) visits at one year were also collected. Clinical follow-up was carried out by local investigators at one year, by medical visit, review of medical history or telephone contact with the patient, family or referring physician.
Statistical Analyses
Categorical variables were expressed as number and percentage. Quantitative variables were expressed as mean and standard deviation in a normal distribution. The normal distribution of quantitative variables was assessed by the Kolmogorov-Smirnoff test. Those quantitative variables with non-normal distribution were expressed as median and interquartile range (25%−75%). For baseline variables, Student t or Mann-Whitney U test was used for comparison of quantitative variables and chi-square test or Fisher's exact test, when appropriate, was used for categorical variables.
Association Between Geriatric Syndromes and Clinical Outcomes
This association was assessed by a Cox regression model, considering the combination of mortality or need for readmission as dependent variable. We assessed the association between frailty as measured by the different tools, disability, cognitive impairment and the rest of geriatric syndromes and the composite of mortality or readmission. The associations between each component of the geriatric assessment and mortality or readmission was considered significant when the P < 0.05 and the 95% CI of the hazard ratio did not include the "1" value. All analysis was performed by PASW Statistics 18 (Chicago, IL, USA).
Ethics
This observational study was performed in accordance with the ethical principles set out in the Declaration of Helsinki. Confidential patient information was protected according to national regulations. The protocol was revised and approved by the Clinical Research Ethics Committee of Bellvitge University Hospital (IRB00005523).
RESULTS
A total of 377 patients were included, with a mean age of 80.4 years (SD 6). Most patents (211/377, 55.9%) were female. The proportion of comorbidities such as hypertension, diabetes mellitus, prior stroke, peripheral artery disease, chronic obstructive pulmonary disease or chronic kidney disease was significant (Table 1).
Table
1.
Clinical characteristics, procedure-related data and geriatric profile in the whole cohort and according to the presence of clinical events during follow up.
Whole population (n = 377)
Patients with mortality or readmission (n = 110)
Patients without events (n = 267)
P-value
Baseline clinical characteristics and procedure related data
Age
80.4 ± 6
80.2 ± 8
80.5 ± 5
0.819
Male gender
166 (44%)
56 (50.9%)
110 (41.2%)
0.018
Hypertension
327 (88.6%)
89 (84.8%)
238 (90.2%)
0.141
Diabetes mellitus
124 (33.6%)
44 (41.9%)
80 (30.3%)
0.023
Dyslipidiemia
290 (78.6%)
84 (80%)
206 (78%)
0.677
Active smoking
11 (2.9%)
4 (3.6%)
7 (2.6%)
0.162
Prior myocardial infarction
26 (7%)
12 (11.4%)
14 (5.3%)
0.044
Prior PCI
58 (15.7%)
21 (20%)
37 (14%)
0.154
Prior cardiac surgery
26 (7%)
6 (5.7%)
20 (7.6%)
0.528
Atrial fibrillation
95(25.2%)
32 (29.1%)
63 (23.6%)
0.207
Prior permanent pacemaker
26 (7%)
9 (8.6%)
17 (6.4%)
0.470
Prior stroke
24 (8.7%)
9 (11.7%)
15 (7.5%)
0.267
Peripheral artery disease
43 (11.7%)
15 (14.3%)
28 (10.6%)
0.326
COPD
39 (14.1%)
13 (16.9%)
26 (13%)
0.405
Chronic kidney disease
137 (37.3%)
43 (41%)
94 (35.9%)
0.364
LEVF
59% ± 9%
59% ± 10%)
59% ± 9%
0.703
Valve In valve
12 (3.3%)
2 (1.9%)
10 (3.8%)
0.283
Pacemaker requirement
65 (18.4%)
24 (23.5%)
41 (16.3%)
0.110
Geriatric assessment
ADL (Barthel Index)
0.283
Independent
232 (61.5%)
63 (57.3%)
169 (63.3%)
Mildly dependent
143 (37.9%)
46 (41.8%)
97 (36.3%)
Instrumental activities (Lawton-Brody index)
0.016
Independent
247 (65.5%)
72 (65.5%)
175 (65.5%)
Mildly dependent
92 (24.4%)
23 (20.9%)
69 (25.8%)
Moderately dependent
28 (7.4%)
7 (6.4%)
21 (7.9%)
Severely dependent
8 (2.1%)
6 (5.5%)
2 (0.7%)
Completely dependent
1 (0.3%)
1 (0.9%)
0
Cognitive impairment (Pfeiffer test)
0.133
None
353 (93.6%)
105 (95.5%)
248 (92.9%)
Mild or moderate
23 (6.1%)
4 (3.6%)
19 (7.1%)
Frailty (Fried criteria)
125 (33.2%)
42 (38.2%)
83 (31.1%)
0.183
Frailty (FRAIL scale)
67 (17.8%)
21 (19.1%)
46 (17.2%)
0.384
Frailty (IF-VIG)
73 (19.5%)
28 (25.7%)
45 (17%)
0.054
Frailty (Essential Frailty Toolset)
0.025
0-1
296 (80%)
79 (74.5%)
217 (82.2%)
2
59 (15.9%)
19 (17.9%)
40 (15.2%)
3
14 (3.8%)
7 (6.6%)
7 (2.7%)
4
1 (0.3%)
1 (0.9%)
0
Frailty (SPPB)
183 (49.2%)
62 (57.9%)
121 (45.7%)
0.032
Data are presented as mean ± SD or n (%). ADL: activities of daily living; IF-VIG: frailty index based on comprehensive geriatric assessment; MNA-SF: mini nutritional assessment-short form.
Patients from this series showed a good physical performance, being most of them independent or mildly dependent both for activities of daily living (ADL) and instrumental activities. Likewise, cognitive status was optimal in the vast majority of patients (Table 1). The proportion of frailty was variable according to the measurement tool used, ranging from 17.6% (FRAIL scale) to 49.8% (SPPB).
Clinical Outcomes at One Year
A total of 20 patients (5.3%) died during the first year after TAVI, mostly due to non cardiac causes (17/20, 85% of deaths). Likewise, 110/377 patients (29.2%) died or were readmitted during the first year. Again, non-cardiac reasons accounted for most readmission episodes. Mean number of readmissions per patient was 0.45 per patient. Mean number of emergency department visits was 0.35 visits per patient.
Clinical Profile of Patients Presenting Death or Readmission at One Year
Patients who died or were readmitted during the first year after the TAVI procedure were more commonly males and had a higher prevalence of comorbidities such as diabetes mellitus and prior myocardial infarction. Age was not significantly different between both groups. The proportion of the rest of comorbidities and procedure-related data were not significantly different regardless of the presence of clinical events during follow up (Table 1).
Impact of Geriatric Syndromes on One-year Clinical Outcomes
Overall, most components of the geriatric assessment showed an association with clinical outcomes at one year (Table 2). Disability for activities of daily living (Barthel Index) was significantly associated with higher mortality and showed a non-significant trend to a higher rate of mortality or readmissions. Barthel Index values were also significantly associated with the number of readmissions in one year, but not with the number of ED visits.
Table
2.
Impact of geriatric syndromes on 1-year clinical outcomes.
Mortality HR (95% CI); P-value
Mortality or readmissionHR (95% CI); P-value
Number readmissions P-value
Number ED visits P-value
Barthel Index
0.943 (0.905−0.982); 0.005
0.98 (0.96−1.01); 0.187
0.005
0.932
Lawton-Brody index
0.739 (0.576−0.948); 0.017
0.81 (0.71−0.91); < 0.001
0.008
0.461
Pfeiffer test
0.045 (0.02−204.2); 0.471
0.99 (0.88-1.71); 0.991
0.588
0.519
Fried criteria
2.60 (1.03−6.59); 0.044
1.35 (0.91−2.01); 0.146
0.261
0.855
FRAIL scale
2.42 (0.91−6.44); 0.078
1.23 (0.75−2.01); 0.414
0.195
0.856
Essential Frailty Toolset
2.21 (0.82−5.99); 0.117
1.44 (0.92−2.24); 0.119
0.003
0.012
SPPB
2.55 (0.9−7.23); 0.079
1.35 (0.91−2); 0.135
0.064
0.837
IF-VIG
518.7 (4.4−61139.3); 0.010
37.5 (2.33−602.4); 0.011
0.001
0.473
ED: emergency department; IF-VIG: Frailty index based on comprehensive geriatric assessment.
Disability for instrumental activities (Lawton-Brody Index) showed a significant association with mortality and a strong association with the rate of mortality or readmission and the number of readmissions. No association was observed between Lawton-Brody index values and the number of ED visits. In contrast, cognitive status (Pfeiffer test) showed no association with any of the components of clinical outcomes at one year.
The association between frailty measurement tools and clinical outcomes was variable, being higher for SPPB, Essential frailty toolset and the IF-VIG tool and lower for Fried criteria and FRAIL scale.
Fried criteria were significantly associated with mortality at one year, but its association with the rate of mortality or readmission, the number of readmissions and ED visits was non-significant. FRAIL scale values showed a non-significant trend to an association with mortality at one year. Again, its association with the rate of mortality or readmission, the number of readmissions and ED visits was non-significant.
The EFT showed a non-significant trend to an association with both mortality and the rate of mortality or readmissions. Its association both with the number of readmissions and the number of ED visits was statistically significant. Likewise, SPPB values showed a non-significant trend to an association with mortality, the rate of mortality or readmissions and the number of readmissions, without any association with the number of ED visits at one year. Finally, IF-VIG values were significantly associated with mortality and the rate of mortality or readmissions, and were strongly associated with the number of readmissions at one year.
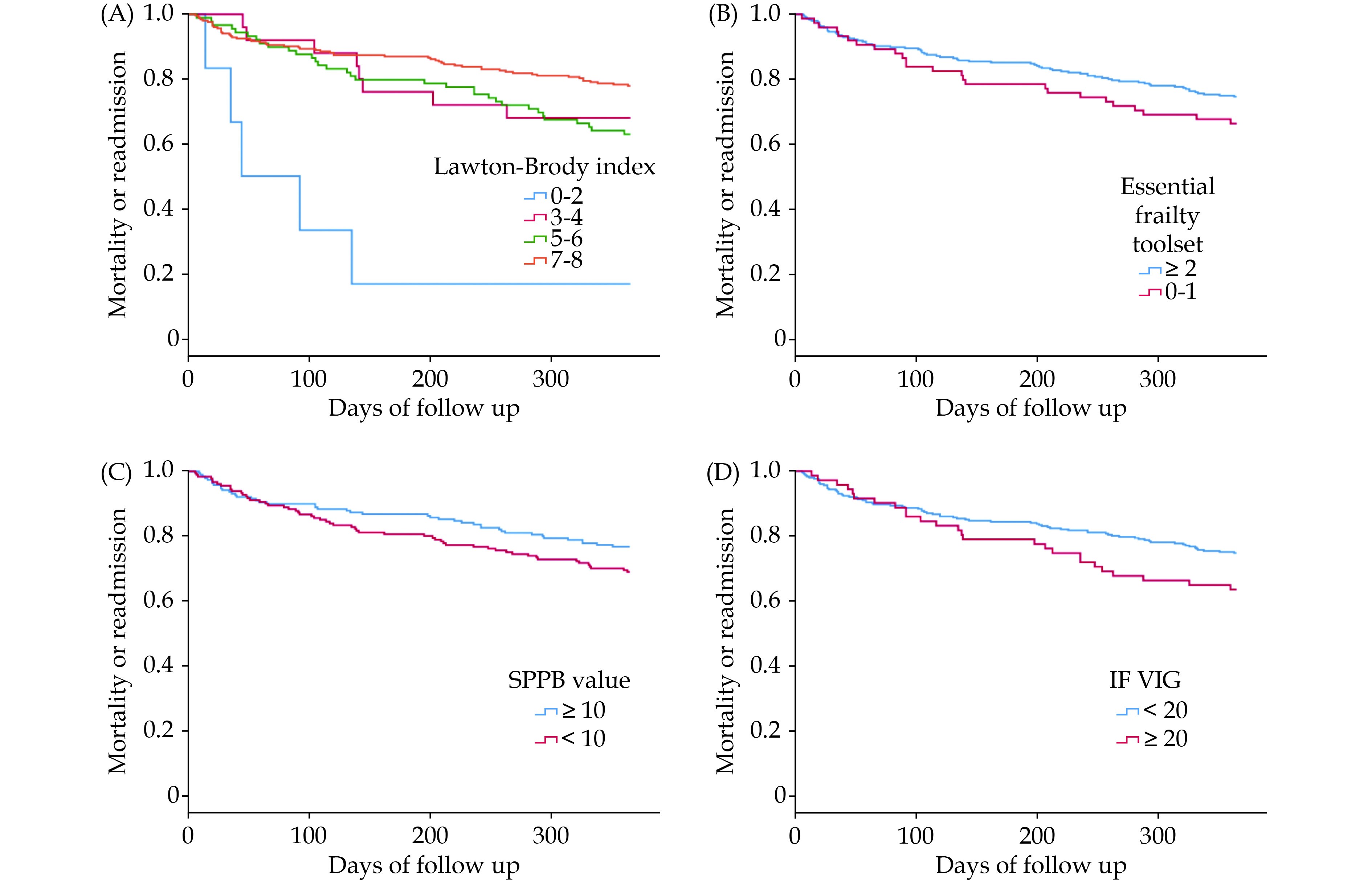
Figure 1 shows the incidence of mortality or readmissions according to (A) disability for instrumental activities, (B) frailty as defined by the Essential frailty toolset, (C) SPPB, and (D) IF-VIG values.
Figure
1.
The incidence of mortality or readmissions according to (A) disability for instrumental activities, (B) frailty as defined by the Essential frailty toolset, (C) SPPB, and (D) IF-VIG values.
IF-VIG: frailty index based on comprehensive geriatric assessment; SPPB: short physical performance battery.
Main findings from our study are: (1) geriatric assessment by the TAVI nurse allowed us to obtain a selected series of older patients with AS with a good physical performance, a very low proportion of cognitive impairment and a reasonably low prevalence of frailty; (2) these patients showed a good clinical course, with a very low rate of mortality at one year and a reasonably low rate of readmissions, mostly due to non cardiac causes; (3) most geriatric assessment tools had an association with a higher rate of clinical events at one year; and (4) the best predictive ability for predicting clinical events was observed for disability for instrumental activities and frailty as measured by the EFT, SPPB and the IF-VIG.
Avoiding futility is one of the main goals when selecting older complex patients with AS for TAVI. In fact, among patients with a higher burden of comorbidities the benefit of TAVI is significantly lower, since these complex patients are at higher incidence of events and mortality due to non cardiac causes that preclude obtaining benefit from treatment.[1] Similar results have been described for interventions such as a routine invasive strategy among frail older patients with acute coronary syndromes.[15,16] Therefore, a routine geriatric assessment before TAVI should contribute to identify patients with an acceptable life expectancy and a reasonably low burden of comorbidities, disability, cognitive impairment and frailty, since this profile of patients might probably obtain a greater benefit from TAVI. Data from our series showed that AS patients treated in our center have very good physical performance (being independent or mildly dependent most of them), with an optimal cognitive status in most cases. The proportion of frailty was slightly higher, ranging from 17.6% to 49% according to the frailty tools used. It is important to note that frailty is a potentially reversible condition at early stages, especially when there is a reversible condition that can increase frailty. In our AS patients a significant part of frailty might be probably due to the cardiac disease, and a significant improvement might be expected after the TAVI procedure.
Probably due to this optimal selection of patients, the rate of one-year clinical events was very low in our series, with a 5% of one year mortality and less than 30% of patients requiring mortality or readmission one year after the TAVI procedure. To our judgement this good clinical course strongly supports the need for maintaining a routine geriatric assessment for optimizing the clinical profile of AS patients undergoing TAVI and their prognosis.
As stated before, geriatric assessment is strongly recommended in this context, but the lack of a clear and agreed-upon assessment is a barrier limiting its use. This lack of consensus surrounding geriatric assessment tools is a major reason why frailty is often not measured in routine clinical practice and why it is reported to have divergent impact across studies.
The most widely validated assessment in clinical practice and with the strongest evidence of benefit is the CGA.[17] This index uses clinical, functional, cognitive, social, and nutritional assessments by different professionals for the design of a treatment and management plan. The CGA is the best diagnostic tool for frailty and provides both an overview and a complete situational diagnosis. However, the main limitations of the CGA are that it is time consuming and requires specialized personnel.
Protocol from our center included the assessment of disability for ADL, instrumental activities, cognitive status and frailty as measured by different tools (Fried criteria, FRAIL scale, EFT, SPPB and the IF-VIG).
The Barthel index is one of the most widely used tools for assessing disability for ADL, and its values are associated both with decision for treatment in complex older patients with AS,[18] and mortality in AS patients after TAVI.[19] Likewise, assessment of disability for instrumental activities is also associated with poorer outcomes among AS patients.[20] Cognitive status is also associated with decision for treatment and outcomes among patients undergoing TAVI.[21] Cognitive assessment was performed by the Pfeiffer test in our protocol, which is a simple screening tool that can be performed in less than 5 min.
Regarding frailty, the Fried scale is one of the most widely used measure of physical frailty. The Fried scale is at intermediate complexity and its values are associated with mortality in AS patients,[22] and with readmission to rehabilitation centers after TAVI.[23] The FRAIL Scale is the easiest tool for measuring frailty; this is a simple-to-use scale that takes less than 2 min to complete as it consists entirely of questions to the patient, with no physical or laboratory tests. The FRAIL scale is an excellent screening tool for an initial assessment frailty, and its values have been associated with poorer outcomes in cardiovascular setting such as acute coronary syndromes.[24] The Short Physical Performance Battery (SPPB) is one of the most recommended physical performance test for frailty in clinical trials. SPPB is of low-to-intermediate complexity, is objective and reproducible, and can be completed in under 5 min. Moreover, in elderly patients with severe AS, frailty assessed with the SPPB shows a correlation with poorer outcomes after TAVI.[25] The EFT includes a short physical test, a cognitive assessment by The Mini Mental State Examination as well as measures of hemoglobin and albumin. While this scale is quite more complex, it has shown an optimal predictive capacity outperforming other frailty scales among older AS patients undergoing valve replacement.[5] Finally, the IF-VIG tool is an intermediate complexity scale that includes 22 questions that can allow a relatively simple, rapid multidimensional assessment and the customization of interventions, among older complex patients in different clinical scenarios. Its ability for predicting outcomes among older patients with AS has not been previously investigated.[26]
Despite the availability of a lot of different scales, there is scarce information about direct comparisons between the predictive ability of these different geriatric assessment tools in older patients with AS. Afilalo, et al[5] analyzed a prospective cohort of 1020 older adults with AS undergoing TAVI or surgical aortic valve replacement (SAVR) from 2012 to 2016, comparing the predictive ability of 7 frailty tools: Fried, Friedþ, Rockwood, Short Physical Performance Battery, Bern, Columbia, and the EFT. Outcomes of interest were all-cause mortality and disability one year after the procedure. Depending on the scale used, the prevalence of frailty ranged from 26% to 68%. Frailty as measured by the EFT was the strongest predictor of death at one year (adjusted odds ratio [OR]: 3.72; 95% CI: 2.54−5.45). Moreover, the EFT was the strongest predictor of worsening disability at one year (adjusted OR: 2.13; 95% CI: 1.57−2.87) and death at 30 days (adjusted OR: 3.29; 95% CI: 1.73−6.26).
Van de Ginste, et al.[25] studied 125 AS patients undergoing TAVI in a single centre retrospective observational study. Psychological, nutritional and physical components of frailty were measured. The primary endpoint was all-cause 1-year mortality. In that study, the nutritional components albumin and Mini-Nutritional Assessment-Short form (MNA-SF) and the physical components gait speed, chair stand test, SPPB, EFT and sarcopenia were associated with increased mortality one year after TAVI. A significant difference in mortality was present if stratified for MNA-SF (P = 0.008), sarcopenia (P < 0.001), SPPB (P = 0.003) and EFT score (P < 0.001). The authors concluded that mainly nutritional and physical components of frailty were associated with 1-year mortality after TAVI.
Data from our study revealed that most geriatric assessment tools were associated with clinical outcomes one year after TAVI in patients. Cognitive status was not associated with any of the components of on year clinical outcomes. This was probably due to the very low proportion of cognitive impairment in our series, because most patients with cognitive decline were previously considered for a conservative approach. Likewise, the proportion of patients with significant disability both for ADL and instrumental activities was very low in our series, being most cases independent or mildly dependent. To our judgement, these data also reflect the grade of selection of our series, considering for treatment only patients with a good physical performance. In contrast to cognitive impairment, disability was associated with clinical events one year after TAVI in our patients, especially for instrumental activities.
Proportion of frailty was variable between the different tools in our series, as observed by other authors.[5] The best ability for predicting outcomes one year after TAVI was observed for EFT, IF-VIG and SPPB. Both SPPB and EFT are strongly recommended tools for frailty assessment in this setting, with a solid association with outcomes as compared to more simple tools such as Fried and FRAIL scale. The good performance of the IF-VIG was also noticeable, since data regarding its use mostly refers to other clinical settings[26] and its ability for predicting outcomes in patients with AS has not been previously described.[27]
To our judgement, this study significantly contributes to select the best tools for frailty assessment in complex patients with AS undergoing TAVI. While the best evidence available supports the use of the EFT, and the SPPB tests, it is also important to note that the presence of disability and the clinical status of the patient are important for selecting frailty assessment tools. In general, scales based on physical frailty should be used for patients with no established disability, whereas scales based on multidimensional frailty (deficit accumulation) are valid for patients with disability. On the other hand, in relatively unstable patients (advanced heart failure, hospital admission) tools that do not need to mobilize patients such as the IF-VIG might have a significant role for frailty assessment.
This study has some limitations, such its retrospective and observational study that preclude excluding selection bias and residual confounding. We only included patients undergoing TAVI and surviving to hospital discharge, so our findings might not be extrapolated to other profile of patients. The sample size of our study was moderate, with few events, and data come from a single centre. Finally, we did not collect information about disability or frailty during follow up.
Despite these limitations, this study retrieves novel and interesting data about geriatric assessment and prognosis among older patients with AS undergoing TAVI. Improving risk stratification, management and outcomes in this continuously growing group of patients might lead to important clinical, economic and social consequences.
Conclusions
Routine geriatric assessment allowed a selection of older patients with AS with a good physical performance, a low proportion of cognitive impairment and a reasonably low prevalence of frailty. These patients showed a good clinical course, with a very low rate of mortality and a reasonably low rate of readmissions at one year. Most geriatric assessment tools had an association with clinical events, but the best predictive ability was observed for disability for instrumental activities and frailty (EFT, SPPB and the IF-VIG).
Martínez-Sellés M, Díez-Villanueva P, Sánchez-Sendin D, et al. PEGASO Registry Group. Comorbidity and intervention in octogenarians with severe symptomatic aortic stenosis. Int J Cardiol 2015; 189: 61−6.
[2]
Richter D, Guasti L, Walker D, et al. Frailty in cardiology: definition, assessment and clinical implications for general cardiology. A consensus document of the Council for Cardiology Practice (CCP), Association for Acute Cardio Vascular Care (ACVC), Association of Cardiovascular Nursing and Allied Professions (ACNAP), European Association of Preventive Cardiology (EAPC), European Heart Rhythm Association (EHRA), Council on Valvular Heart Diseases (VHD), Council on Hypertension (CHT), Council of Cardio-Oncology (CCO), Working Group (WG) Aorta and Peripheral Vascular Diseases, WG e-Cardiology, WG Thrombosis, of the European Society of Cardiology, European Primary Care Cardiology Society (EPCCS). Eur J Prev Cardiol 2022; 29: 216−227.
[3]
Vahanian A, Beyersdorf F, Praz F, et al. ESC/EACTS Scientific Document Group. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J 2022; 12;43: 561−632.
[4]
Gary R. Evaluation of frailty in older adults with cardiovascular disease: incorporating physical performance measures. J Cardiovasc Nurs 2012; 27: 120−31. doi: 10.1097/JCN.0b013e318239f4a4
[5]
Afilalo J, Lauck S, Kim DH, et al. Frailty in Older Adults Undergoing Aortic Valve Replacement: The FRAILTY-AVR Study. J Am Coll Cardiol 2017; 70: 689−700. doi: 10.1016/j.jacc.2017.06.024
[6]
Shimura T, Yamamoto M, Kano S, et al. Impact of the clinical frailty scale on outcomes after transcatheter aortic valve replacement. Circulation 2017; 135: 2013−2024. doi: 10.1161/CIRCULATIONAHA.116.025630
[7]
Díez-Villanueva P, Arizá-Solé A, Vidán MT, et al. Recommendations of the Geriatric Cardiology Section of the Spanish Society of Cardiology for the Assessment of Frailty in Elderly Patients With Heart Disease. Rev Esp Cardiol (Engl Ed) 2019; 72: 63−71. doi: 10.1016/j.recesp.2018.06.015
[8]
Mahoney FI, Barthel DW. Functional evaluation: the Barthel Index. Md Med J 1965; 14: 61−65.
[9]
Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities daily living. Gerontologist 1969; 9: 179−86. doi: 10.1093/geront/9.3_Part_1.179
[10]
Pfeiffer E. A short portable mental status questionnaire for the assessment of organic brain deficit in elderly patients. J Am Geriatr Soc 1975; 23: 433−441. doi: 10.1111/j.1532-5415.1975.tb00927.x
[11]
Guralnik JM, Simonsick EM, Ferrucci L, et al. A short physical performance battery assessing lower extremity function: association with selfreported disability and prediction of mortality and nursing home admission. J Gerontol 1994; 49: 85−94.
[12]
Abellan van Kan G, Rolland Y, Bergman H et al. The I. A. N. A. Task force on frailty assessment of older people in clinical practice. J Nutr Health Aging 2008; 12: 29−37.
[13]
Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci 2001; 56: 146−156. doi: 10.1093/gerona/56.3.M146
[14]
Amblàs-Novellas J, Martori JC, Molist Brunet N, et al. [Frail-VIG index: Design and evaluation of a new frailty index based on the Comprehensive Geriatric Assessment]. Rev Esp Geriatr Gerontol 2017; 52: 119−127. [Article in Spanish]. doi: 10.1016/j.regg.2016.09.003
[15]
Sanchis J, Núñez E, Barrabés JA, et al. Randomized comparison between the invasive and conservative strategies in comorbid elderly patients with non-ST elevation myocardial infarction. Eur J Intern Med 2016; 35: 89−94. doi: 10.1016/j.ejim.2016.07.003
[16]
Sanchis J, Bueno H, Miñana G, et al. Effect of Routine Invasive vs Conservative Strategy in Older Adults With Frailty and Non-ST-Segment Elevation Acute Myocardial Infarction: A Randomized Clinical Trial. JAMA Intern Med 2023; 183: 407−415. doi: 10.1001/jamainternmed.2023.0047
[17]
Ellis G, Whitehead MA, O’Neill D, et al. Comprehensive geriatric assessment for older adults admitted to hospital. Cochrane Database Syst Rev 2011; 9: CD006211.
[18]
Solla P, Díaz R, Herrera J, et al. Cognitive impairment in the elderly patient with symptomatic severe aortic stenosis. Therapeutic decisions and impact on one-year mortality]. Rev Neurol 2023; 76: 127−135.
[19]
Tarro Genta F, Marcassa C, Ceresa M, et al. Predictors of survival in patients undergoing cardiac rehabilitation after transcatheter aortic valve replacement (TAVR): a multicenter retrospective study. Panminerva Med 2023; 65: 220−226.
[20]
Piñon M, Paredes E, Acuña B, et al. Frailty, disability and comorbidity: different domains lead to different effects after surgical aortic valve replacement in elderly patients. Interact Cardiovasc Thorac Surg 2019; 29: 371−377. doi: 10.1093/icvts/ivz093
[21]
El-Sabawi B, Cloud H, Patel JN, et al, Association of Depression and Cognitive Dysfunction With Patient-Centered Outcomes After Transcatheter Aortic Valve Replacement. Circ Cardiovasc Interv 2023; 16: e012875.
[22]
Rodriguez-Pascual C, Paredes-Galán E, Ferrero-Martínez AI, et al. The frailty syndrome and mortality among very old patients with symptomatic severe aortic stenosis under different treatments. Int J Cardiol 2016; 224: 125−131. doi: 10.1016/j.ijcard.2016.09.020
[23]
Huded CP, Huded JM, Friedman JL, et al. Frailty status and outcomes after transcatheter aortic valve implantation. Am J Cardiol 2016; 117: 1966−1971. doi: 10.1016/j.amjcard.2016.03.044
[24]
Alegre O, Formiga F, López-Palop R, et al. LONGEVO-SCA registry investigators. An Easy Assessment of Frailty at Baseline Independently Predicts Prognosis in Very Elderly Patients With Acute Coronary Syndromes. J Am Med Dir Assoc 2018; 19: 296−303.
[25]
Van de Velde-Van De Ginste S, Perkisas S, Vermeersch P, et al. Physical components of frailty in predicting mortality after transcatheter aortic valve implantation (TAVI). Acta Cardiol 2021; 76: 681−688. doi: 10.1080/00015385.2020.1769346
[26]
Gutiérrez Jiménez N, Satué-Gracia E, Contel JC, et al. Feasibility, Reliability, and Validity of the VIG-Express Questionnaire as an Instrument for Rapid Multidimensional Geriatric Assessment: A Multicenter Study. Aten Primaria 2024; 57: 103108.
[27]
Badosa-Collell G, Latorre-Vallbona N, Martori JC et al. Capacidad predictiva de mortalidad del índice Frágil-VIG (IF-VIG) en pacientes ancianos con fractura de fémur. Rev Esp Geriatr Gerontol 2022; 57: 220−223. doi: 10.1016/j.regg.2022.05.002
Table
1.
Clinical characteristics, procedure-related data and geriatric profile in the whole cohort and according to the presence of clinical events during follow up.
Whole population (n = 377)
Patients with mortality or readmission (n = 110)
Patients without events (n = 267)
P-value
Baseline clinical characteristics and procedure related data
Age
80.4 ± 6
80.2 ± 8
80.5 ± 5
0.819
Male gender
166 (44%)
56 (50.9%)
110 (41.2%)
0.018
Hypertension
327 (88.6%)
89 (84.8%)
238 (90.2%)
0.141
Diabetes mellitus
124 (33.6%)
44 (41.9%)
80 (30.3%)
0.023
Dyslipidiemia
290 (78.6%)
84 (80%)
206 (78%)
0.677
Active smoking
11 (2.9%)
4 (3.6%)
7 (2.6%)
0.162
Prior myocardial infarction
26 (7%)
12 (11.4%)
14 (5.3%)
0.044
Prior PCI
58 (15.7%)
21 (20%)
37 (14%)
0.154
Prior cardiac surgery
26 (7%)
6 (5.7%)
20 (7.6%)
0.528
Atrial fibrillation
95(25.2%)
32 (29.1%)
63 (23.6%)
0.207
Prior permanent pacemaker
26 (7%)
9 (8.6%)
17 (6.4%)
0.470
Prior stroke
24 (8.7%)
9 (11.7%)
15 (7.5%)
0.267
Peripheral artery disease
43 (11.7%)
15 (14.3%)
28 (10.6%)
0.326
COPD
39 (14.1%)
13 (16.9%)
26 (13%)
0.405
Chronic kidney disease
137 (37.3%)
43 (41%)
94 (35.9%)
0.364
LEVF
59% ± 9%
59% ± 10%)
59% ± 9%
0.703
Valve In valve
12 (3.3%)
2 (1.9%)
10 (3.8%)
0.283
Pacemaker requirement
65 (18.4%)
24 (23.5%)
41 (16.3%)
0.110
Geriatric assessment
ADL (Barthel Index)
0.283
Independent
232 (61.5%)
63 (57.3%)
169 (63.3%)
Mildly dependent
143 (37.9%)
46 (41.8%)
97 (36.3%)
Instrumental activities (Lawton-Brody index)
0.016
Independent
247 (65.5%)
72 (65.5%)
175 (65.5%)
Mildly dependent
92 (24.4%)
23 (20.9%)
69 (25.8%)
Moderately dependent
28 (7.4%)
7 (6.4%)
21 (7.9%)
Severely dependent
8 (2.1%)
6 (5.5%)
2 (0.7%)
Completely dependent
1 (0.3%)
1 (0.9%)
0
Cognitive impairment (Pfeiffer test)
0.133
None
353 (93.6%)
105 (95.5%)
248 (92.9%)
Mild or moderate
23 (6.1%)
4 (3.6%)
19 (7.1%)
Frailty (Fried criteria)
125 (33.2%)
42 (38.2%)
83 (31.1%)
0.183
Frailty (FRAIL scale)
67 (17.8%)
21 (19.1%)
46 (17.2%)
0.384
Frailty (IF-VIG)
73 (19.5%)
28 (25.7%)
45 (17%)
0.054
Frailty (Essential Frailty Toolset)
0.025
0-1
296 (80%)
79 (74.5%)
217 (82.2%)
2
59 (15.9%)
19 (17.9%)
40 (15.2%)
3
14 (3.8%)
7 (6.6%)
7 (2.7%)
4
1 (0.3%)
1 (0.9%)
0
Frailty (SPPB)
183 (49.2%)
62 (57.9%)
121 (45.7%)
0.032
Data are presented as mean ± SD or n (%). ADL: activities of daily living; IF-VIG: frailty index based on comprehensive geriatric assessment; MNA-SF: mini nutritional assessment-short form.



 DownLoad:
DownLoad: